
Ahmed Nabil
Moderators
-
Joined
-
Last visited
-
long/short is a better word. The Higher the defect ,The shorter the COMMON WALL & The LOWER the defect the longer the Common wall
-
-
 @FARID Pneumoperitoneum is the only absolute indication to go for surgery in NEC. in cases without Pneumoperitoneum, it is a difficult decision to go for surgery and MD7 criteria may help.
@FARID Pneumoperitoneum is the only absolute indication to go for surgery in NEC. in cases without Pneumoperitoneum, it is a difficult decision to go for surgery and MD7 criteria may help.- 1 comment
- 2 reviews
-
-

- 1
-
-
 @FARID personally I do anal calibration 2 weeks post pull through, and I may dilate if needed
@FARID personally I do anal calibration 2 weeks post pull through, and I may dilate if needed -
 @FARID Timing of UDT repair when associated with hypospadias depend on type of hypospadias and the anticipation of the need for tunica vaginals flap during hypospadias repair.
@FARID Timing of UDT repair when associated with hypospadias depend on type of hypospadias and the anticipation of the need for tunica vaginals flap during hypospadias repair. -
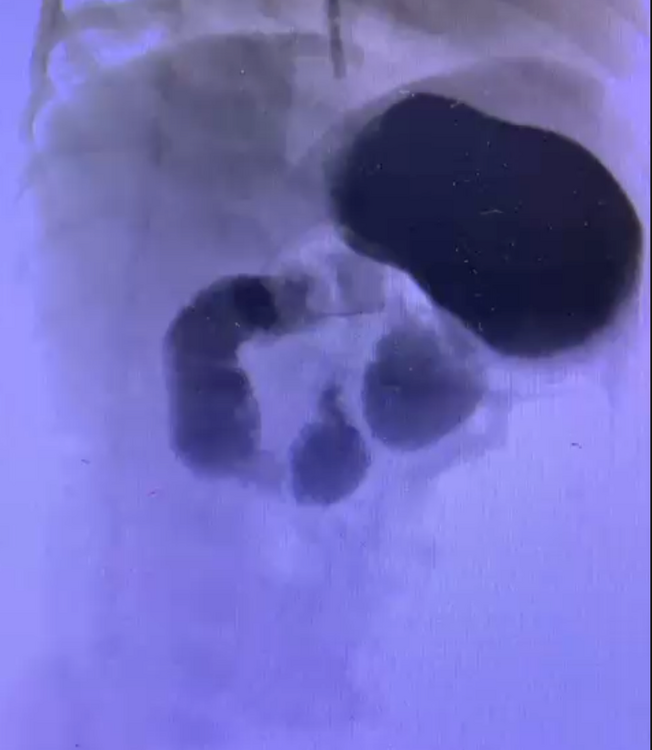
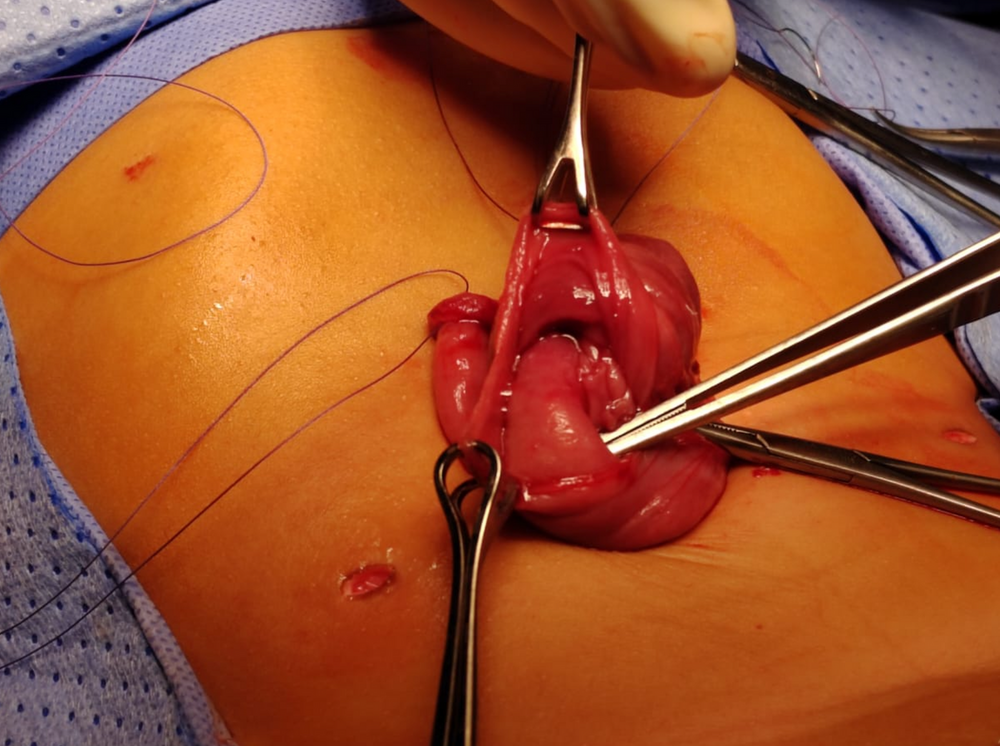
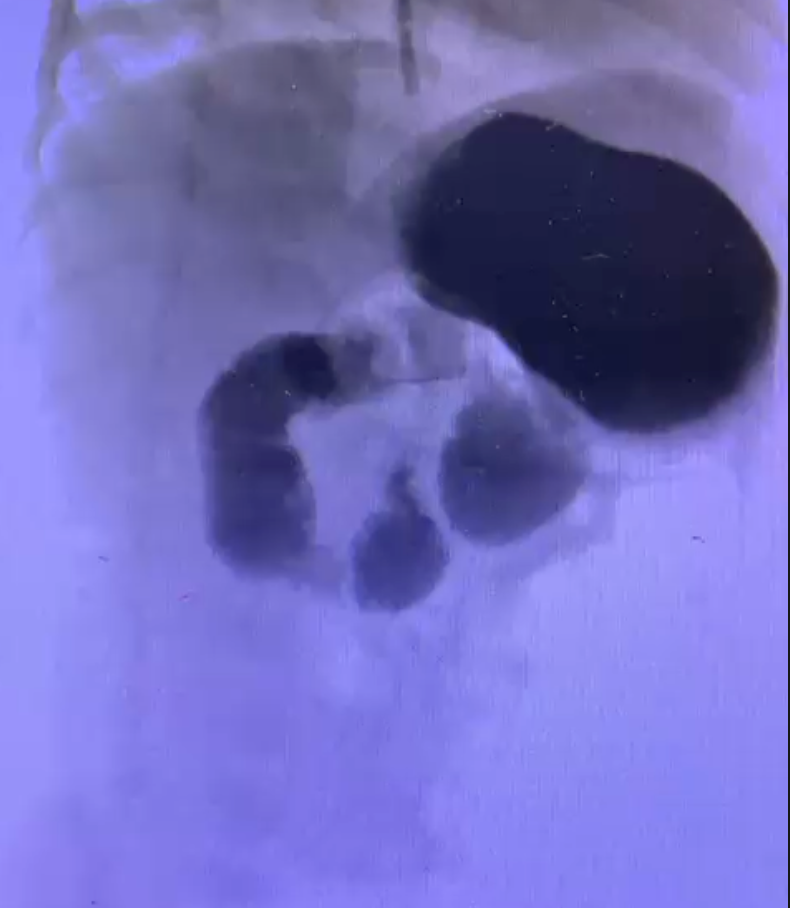
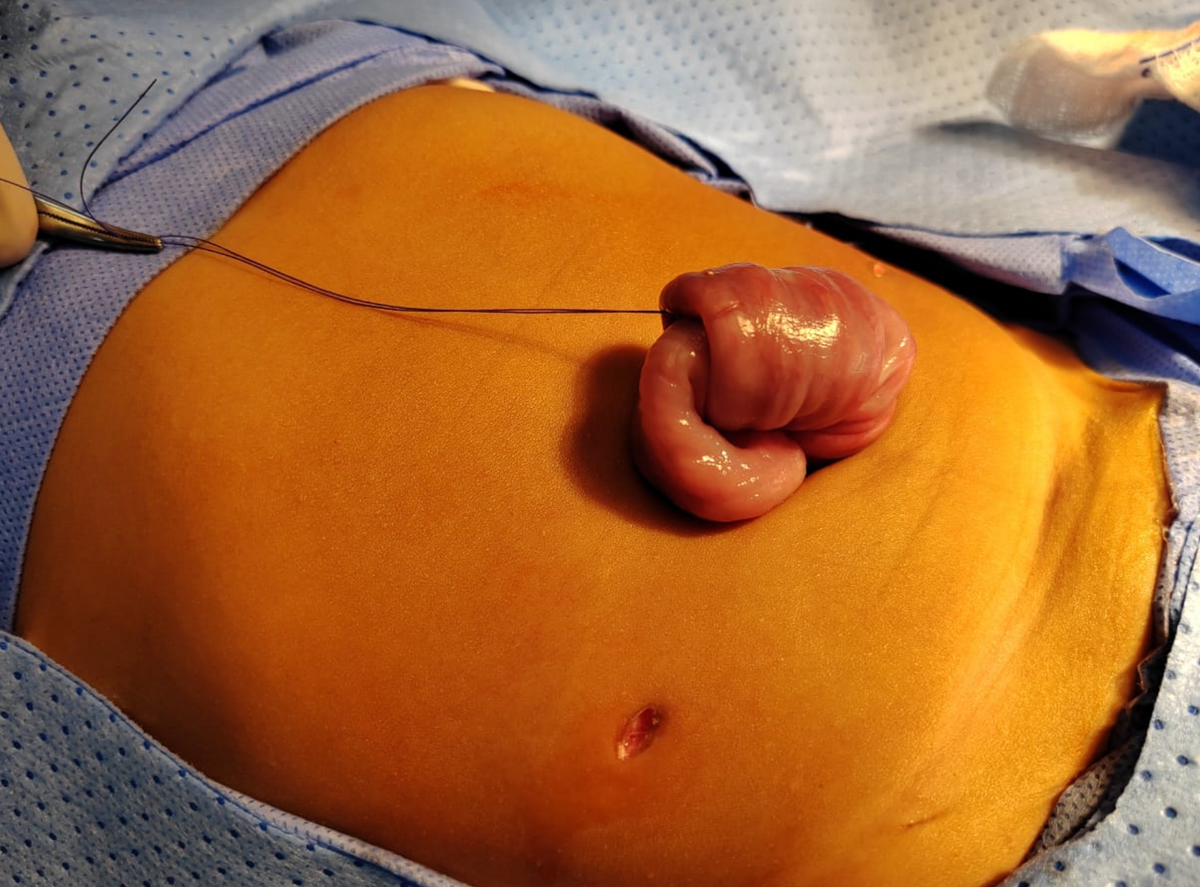
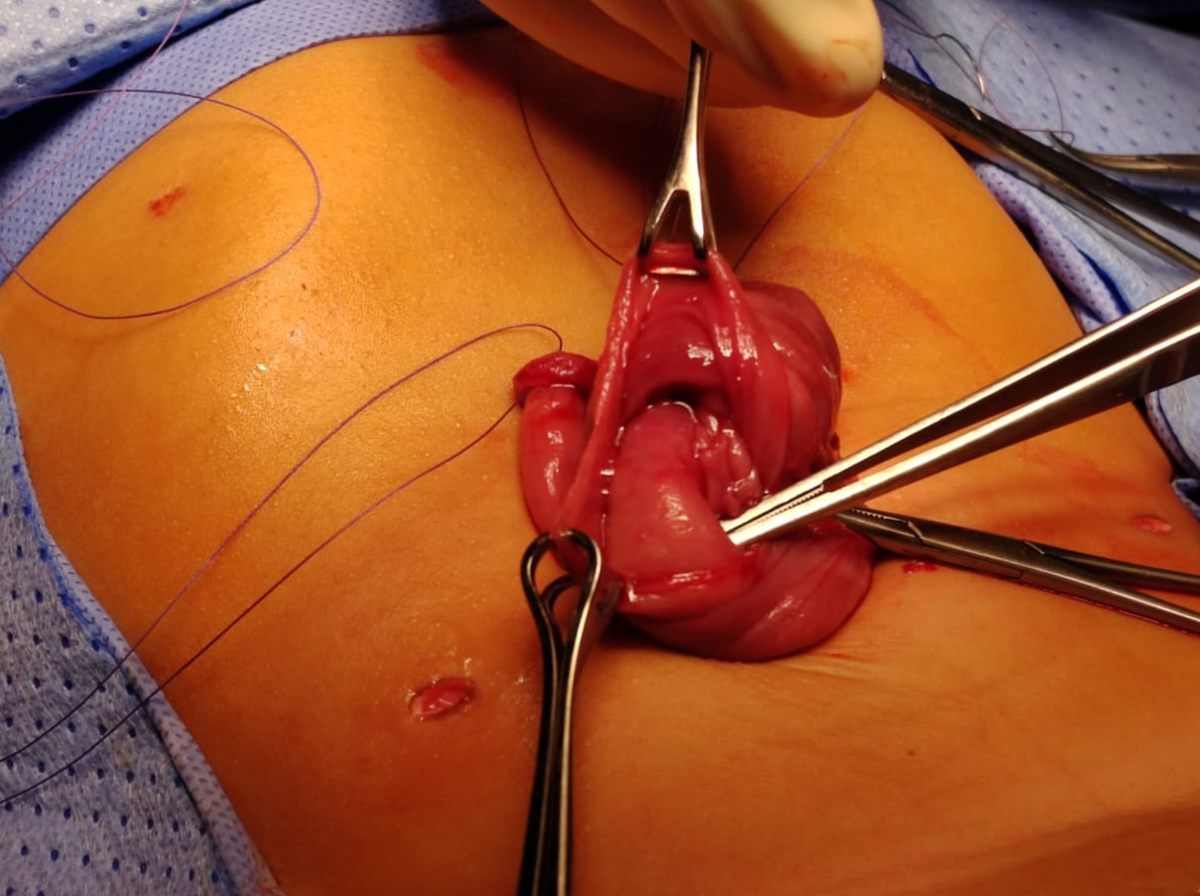
case of prof Tariq Altokais from KKUH, Riyadh, Saudi Arabia. a case of female patient 8m old with black tarry stool since the age of 4m, and on/off milk reflux/vomiting. +ve occult blood in stool, patient is failing to thrive (current weight 6.1kg), -ve Meckel scan and was prepared for upper GI endoscopy by pediatric GI team. presented suddenly two days ago with persistent dark bilious vomiting of large amount. abdominal u/s done and was negative, upper GI contrast study revealed arrest of dye at DJ junction at the time of study, with passage of contrast in the after 1 hrs delayed film. diagnostic laparoscopy done for the patient and a proximal jejunal intussception found just distal to DJ junction, which reduced laparoscopcally, and we found a suspicious thickened dilated segment of proximal jejunum, then umclical incision extended and this jejunal segment delivered outside the abdomen and opened to find a intraluminal polyp, resection anastomosis done. Pathology result: hamartomatus polyp



-
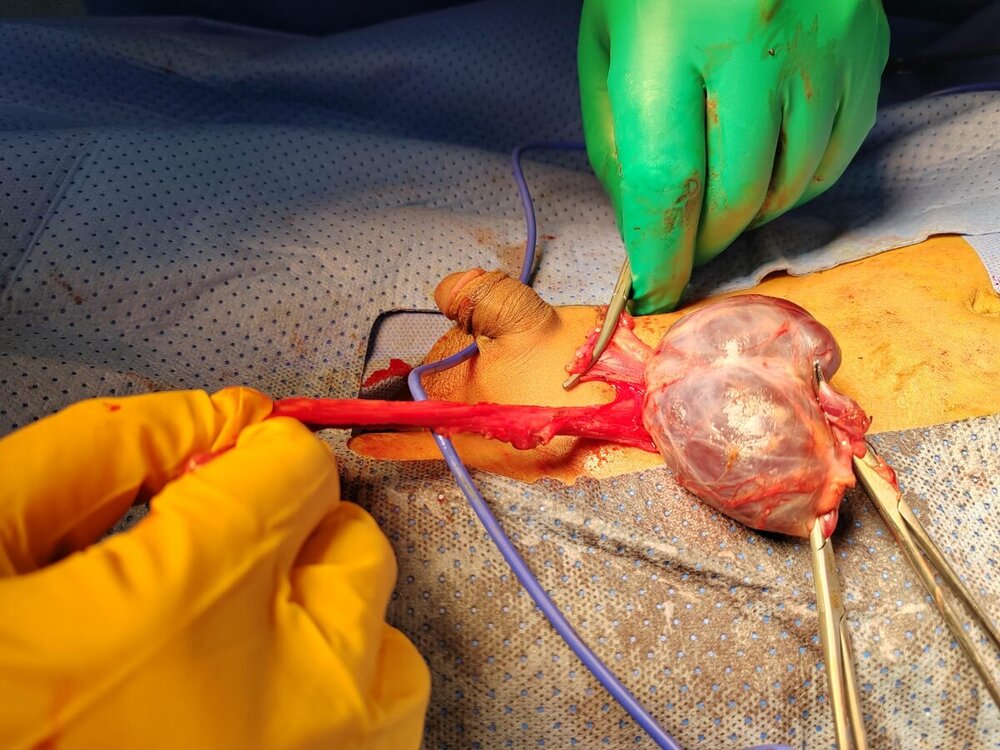
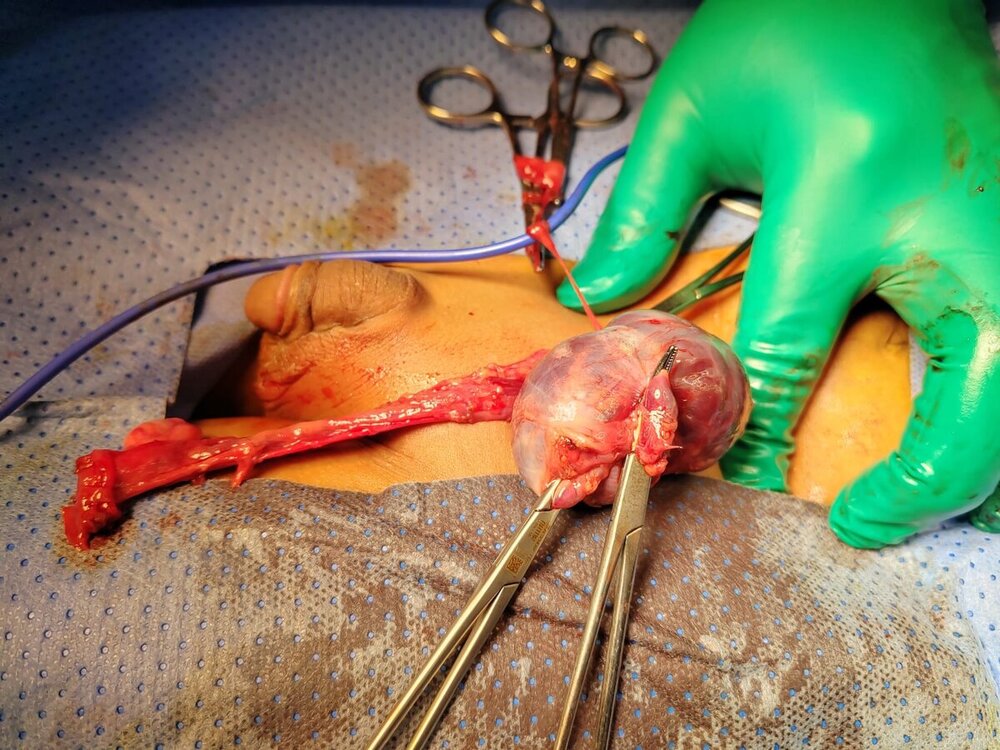
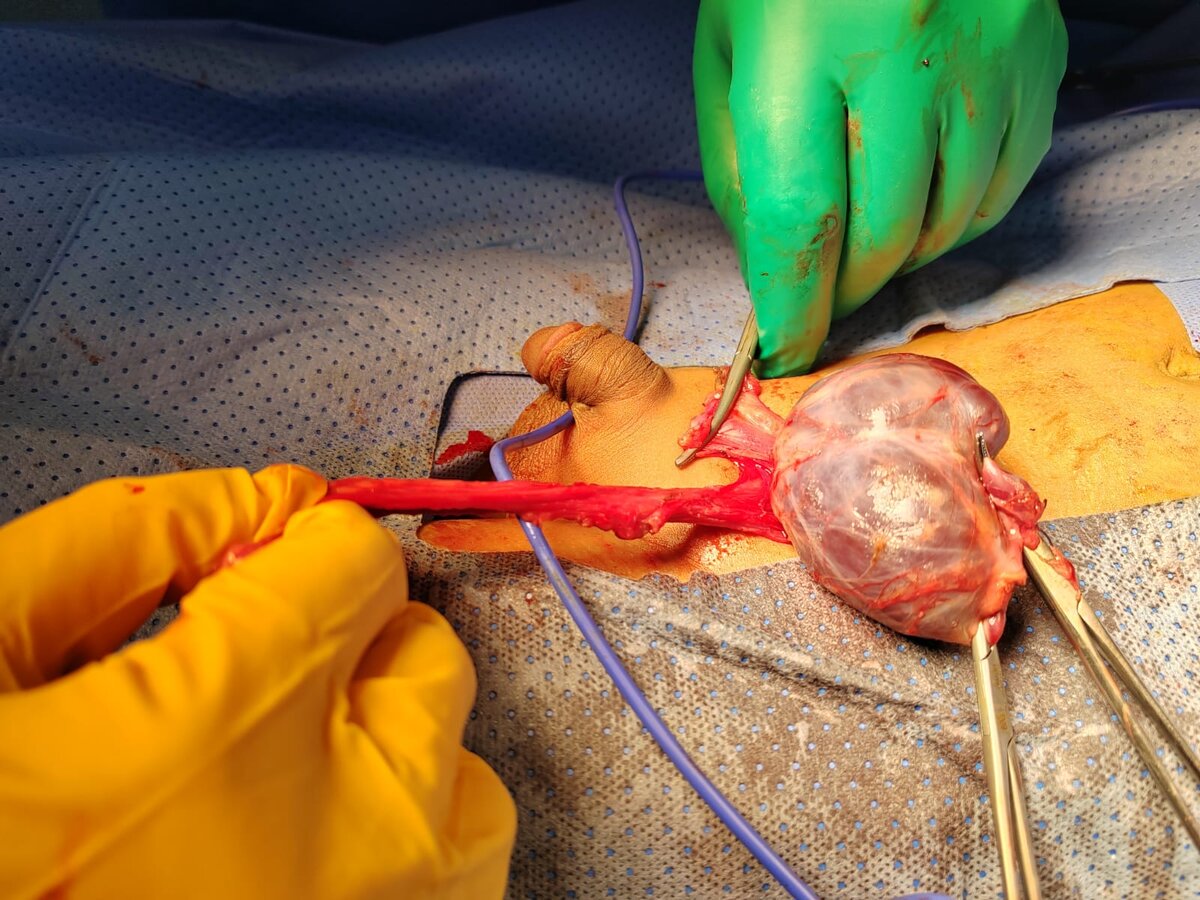
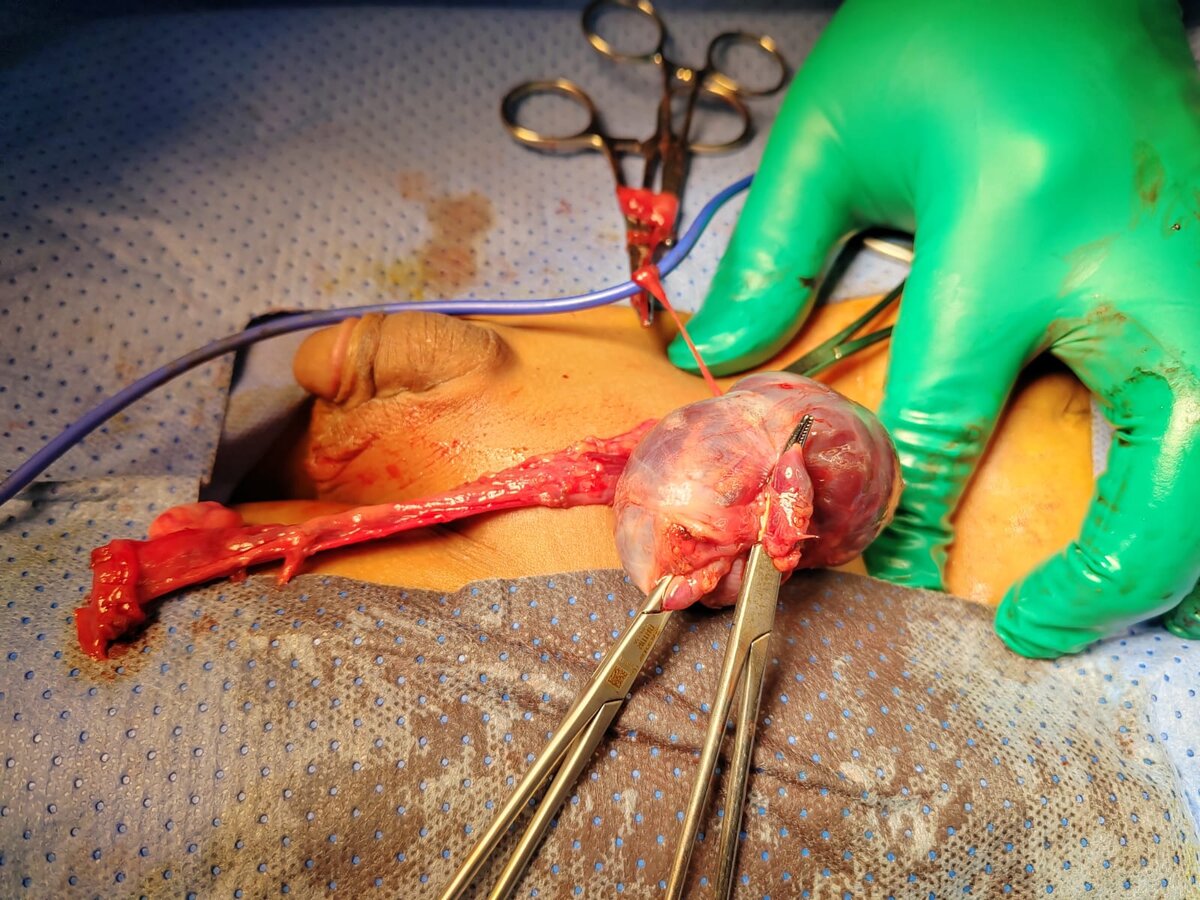
Thank you for your questions 1- this discovered intraoperatively 2- no risk factors identified 3- presentation is left inguinal hernia 4- there was associated big left hernia sac 5- no bleeding source identified (bleeding was inside abdominal hydrocele, no history of trauma!?!)
-
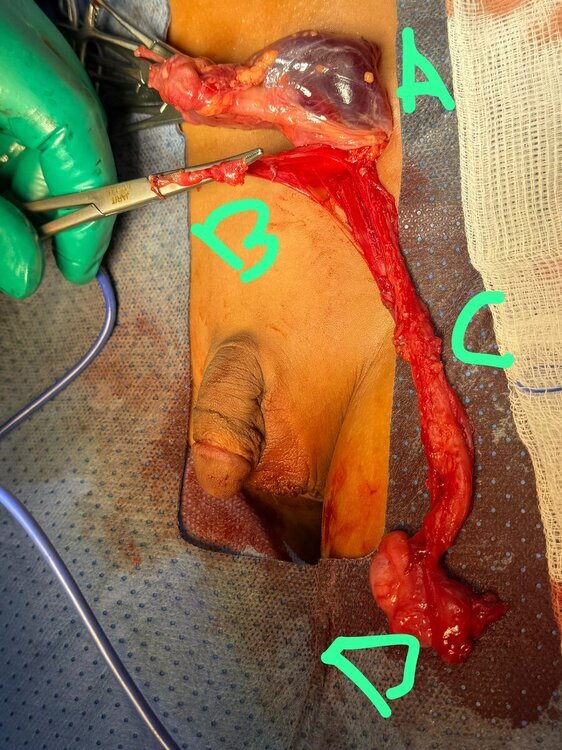
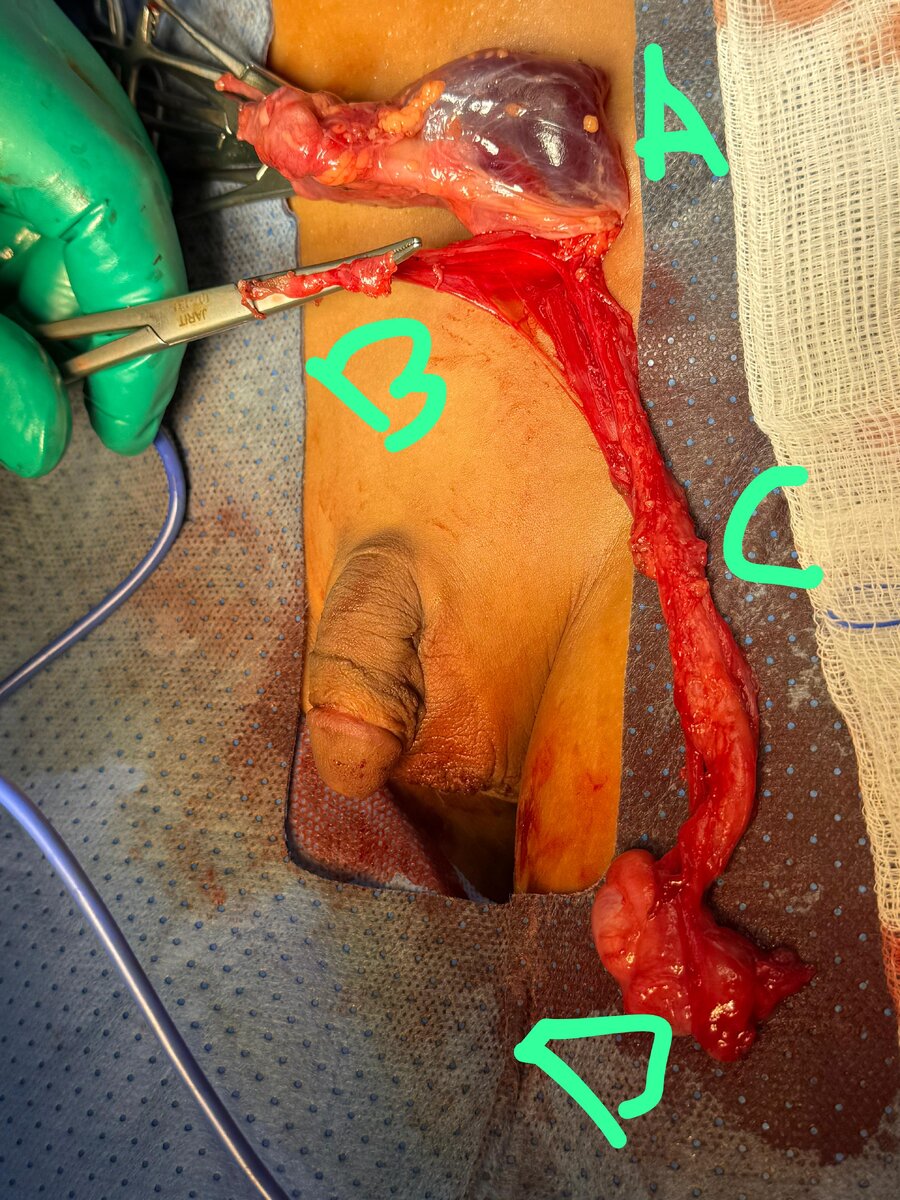
A case of left abdomenoscrotal hematocele in a three yrs old patient, originally operated for left UDT with left inguinal hernia. operated through groin incision A abdominal part of hematocele delivered to groin B inguinal hernial sac C cord including vas and vessel D Lt testis
.thumb.jpeg.caf2f6389ac7e4ba03304a934ebc2988.jpeg)

.thumb.jpeg.b1e21e13d4ac36756add09a0e9aa17e1.jpeg)



.jpeg.c14eebe0f4b4be76454c8dab961e98da.jpeg)

.jpeg.3c312ea62a88e58e6d7416bdbe3797c5.jpeg)