admin
Administrators
-
Joined
-
Last visited
Everything posted by admin
-
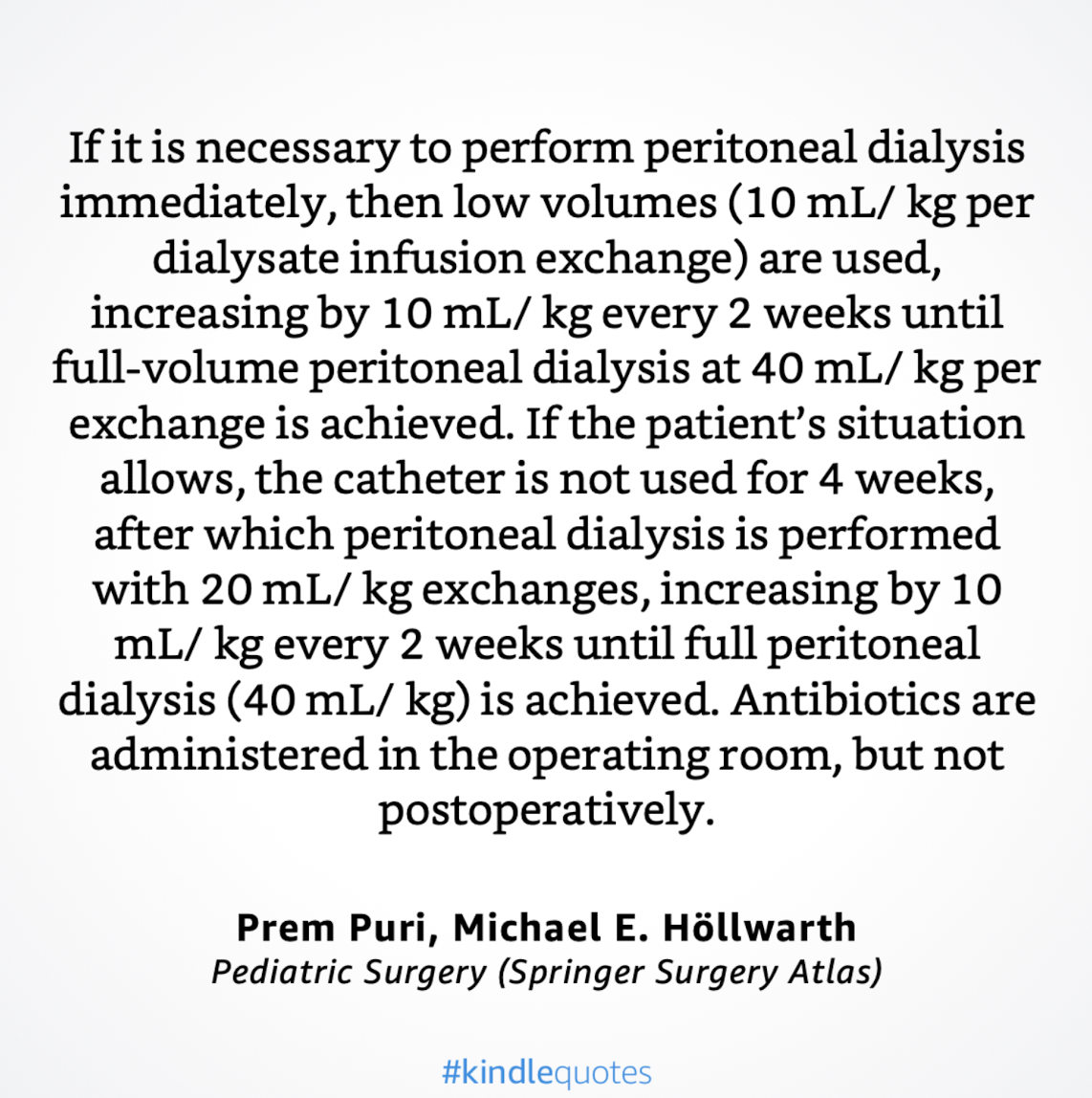
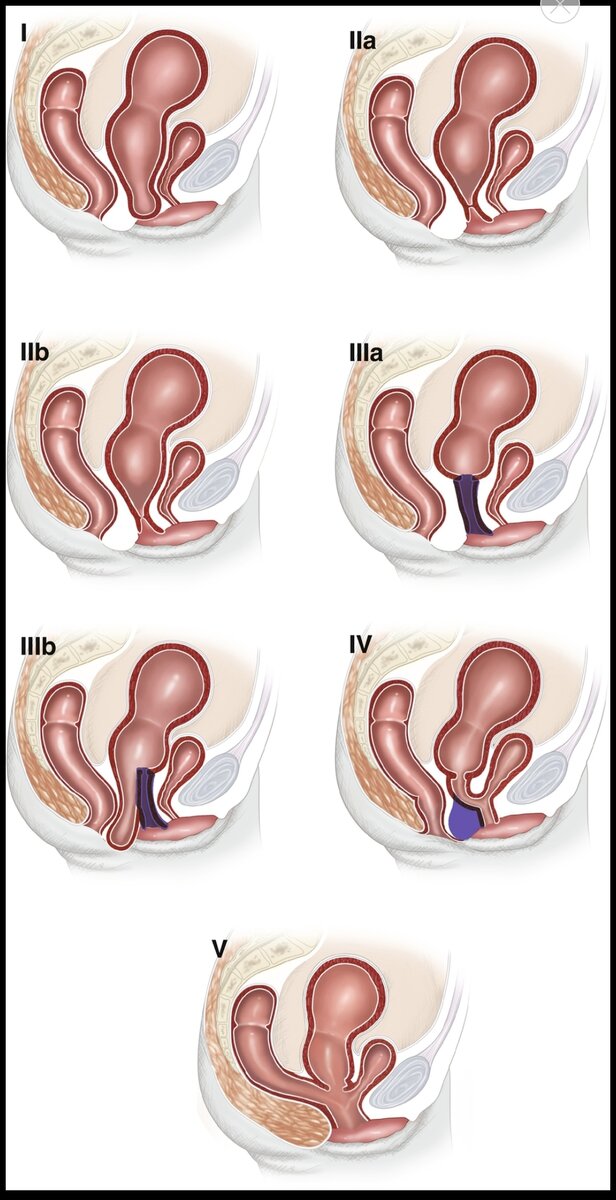
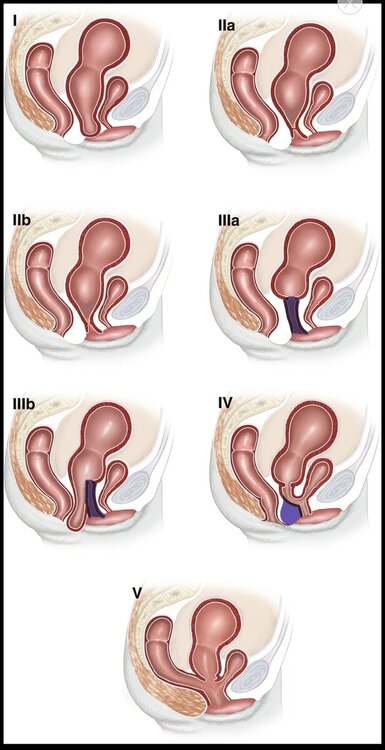
quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Hydrometrocolpos has been classified into five types (Fig. 73.1) on the basis of the type and level of obstruction: 1. Low hymenal obstruction. 2. Mid-plane transverse membrane or septum. (a) Without communication. (b) With a small orifice as communication. 3. High obstruction with distal vaginal atresia. (a) Without perineal swelling. (b) With perineal swelling. 4. Vaginal atresia with persistence of the urogenital sinus. 5. Vaginal atresia with cloacal anomaly."
 quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Hydrometrocolpos presents at the two extremes of childhood: initially during the neonatal period, when there is a high level of maternal hormones, and then at early puberty, when the patient herself begins to have production of estrogenic hormones. The distal vaginal obstruction is mostly due to imperforate hymen (in two thirds of cases), followed by a transverse vaginal septum and less commonly, vaginal atresia (with or without persistence of a urogenital sinus or cloaca)." "Associated anomalies are common and quite often severe. These include anorectal malformations and unilateral or bilateral agenesis of the kidneys, ureters, and trigone. Ultrasonography, micturating cystourethrography (MCU), and MR urography can help to evaluate the associated genitourinary anomalies."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Several problems have been encountered during the establishment of the ACE. The most common is pain during the washout, which is reported in up to 60% of patients. This usually settles spontaneously during the first 3 months but can be helped by reducing the concentration of the phosphate, reducing the rate of the infusion, or using an antispasmodic prior to the enema (such as Colofac, Solvary, UK). Despite regular washouts, patients may still become constipated, which also produces pain and should always be excluded. One of the other problems encountered is the time taken for the enema to pass and achieve a result; this has been a significant contributory factor to failure. The placement of the conduit in the distal descending colon has improved this situation considerably. Patients in whom the standard caecal ACE did not work have achieved excellent results with the left colonic ACE."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "None of our patients have needed secondary augmentation because of increased contractile activity. Even after the ileal segment is isolated from the gastrointestinal tract, it retains its absorption and secretory properties. As a result of the electrolyte exchange, hyperchloremic metabolic acidosis may develop. The extent of the electrolyte exchange depends on the amount of intestinal surface area in contact with urine and the time that the urine remains in contact with the intestine. Patients with normal renal function prior to augmentation have adequate compensatory mechanisms and do not have significant problems with acute metabolic changes. Patients who develop persistent, severe metabolic changes must be evaluated for insufficient bladder emptying. Another concern in these patients is a possible increased incidence of urinary tract infection (UTI), as bacterial flora from the augmentation may colonize the urinary tract. In recent years, we have used in our patients daily irrigation of the augmented bladder with 30 mL of 120 mg gentamicin per 250 mL of normal saline, and have found a low incidence of UTI with no evidence of gentamicin absorption or renal function deterioration."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "The site of the stoma on the skin is selected entirely for the patient’s convenience. The umbilicus provides a good passage and the best cosmetic result, but it is not an option in exstrophy patients. With patients in wheelchairs, the spine tends to become twisted with time, causing progressive abdominal compression, and the abdomen becomes hidden from the patient’s field of vision. For these patients, a stoma site close to the xiphisternum is the best option."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Augmentation cystoplasty is now commonly performed at most pediatric urological centres. Bladder augmentation has three major goals: to provide a compliant bladder reservoir, to limit bladder contractility, and to increase bladder capacity. Augmentation cystoplasty should allow the urinary tract to remain intact while preserving renal function and providing urinary continence. Various substrates are utilized to augment the bladder; the most commonly used is a segment of ileum, but stomach and large bowel also have been used. Ileum has been demonstrated to be the least contractile segment and therefore has become the tissue most often used for bladder augmentation. Sufficient augmentation should lead to effective bladder capacity."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Successful initial closure of the bladder and posterior urethra is the most important factor for achieving urinary continence and sufficient bladder capacity. The fragile mucosa and the detrusor function are best preserved by closing the bladder in the newborn period, but the size and the functional capacity of the detrusor muscle are important considerations for the outcome. Therefore, in the rare presence of a small, fibrotic bladder patch without elasticity or contractility, the operation should be deferred until adequate growth of the bladder template occurs. The risk of bladder neck failure is higher for the group with smaller bladder capacities (<100 mL). If sufficient size is not reached 4–6 months after birth, alternative options like creation of a colon conduit or ureterosigmoidostomy must be employed. Later in life, the former urinary diversion can be converted into a continent catheterizable pouch bladder or augmented bladder if the template is still intact."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Before the operation, the bladder capacity is measured annually by gravity cystograms with the child in anaesthesia. A bladder capacity of 100 mL or more is necessary to undergo bladder neck reconstruction. All children undergo an intense voiding training program, along with urodynamic evaluation, prior to the reconstruction."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "The ureteral stents are left in place for 10–14 days, and the suprapubic tube is removed 4 weeks postoperatively, after calibrating the bladder outlet to warrant free drainage. Note that the urethra is not stented at the end of the operation to avoid pressure necrosis, infection, and secretion accumulation. The pelvis is approximated in the midline by gently applying pressure over the greater trochanters bilaterally. Horizontal mattress sutures of #2 nylon are placed in the pubis. It is important to tie the knot away from the neourethra to avoid material migration into the posterior urethra. A second stitch of #2 nylon is used at the most caudal insertion of the rectus fascia onto the pubic bone for added security, if it can be easily done and does not compromise the first stitch."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "The operations are performed with general anaesthesia, with the patient in a supine position even for the osteotomies. A tunneled epidural catheter is placed when possible to reduce the intraoperative amount of anaesthetic agents and for postoperative pain control. It is typically left in place for several weeks after the closure. Care must be taken to create a latex-free environment in the operation room, as many children with bladder exstrophy are prone to latex allergies. Perioperative broad-spectrum antibiotics are administered and continued throughout the first postoperative week."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Combined exstrophy and epispadias repair: In a few selected cases, newborn exstrophy closure can be combined with epispadias repair. This approach requires good phallic length, a deep urethral groove, and an adequate amount of penile skin, however, and it should be attempted only by experienced exstrophy surgeons, as the complications can be severe. Combined exstrophy and epispadias repair is best applied in the patient undergoing delayed primary or reoperative exstrophy closure. The preoperative use of intramuscular testosterone in reoperative exstrophy patients will allow for improved vascularity and more penile skin for the reconstruction."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "pelvic osteotomies are performed if the patient is older than 72 h, for a symphyseal diastasis of more than 4 cm or if a tension-free closure cannot be achieved. In those cases, osteotomies are crucial to ensure tension-free approximation of the bladder, posterior urethra, and abdominal wall, preventing dehiscence or bladder prolapse. Furthermore, it places the urethra deep within the pelvic ring, enhances bladder outlet resistance, and ensures alignment of the large pelvic floor muscles to support the bladder neck."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Achieving urinary continence with a sufficient bladder capacity is strongly dependent on initial successful closure of the bladder and the posterior urethra as well as the size of the bladder template. Therefore, the first step of the reconstruction is conversion of bladder exstrophy into a penile epispadias with incontinence with a balanced posterior outlet resistance that preserves renal function but stimulates bladder growth."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "The technique includes early closure of the bladder, posterior urethra, and abdominal wall, usually with pelvic osteotomy in the newborn period, subsequently followed by an early epispadias repair at 6 months to 1 year of age after testosterone stimulation by intramuscular injection. Around age 4–5 years, when adequate bladder capacity is reached and the child is ready to participate in a very structured preoperative and postoperative voiding program, a competent bladder neck is reconstructed, with bilateral ureteral reimplantation."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Ureteral reflux in various degrees is seen in 100% of cases after closure. A preoperative ultrasound evaluation of the otherwise usually unaffected upper tracts is mandatory to determine the presence of two normal kidneys"video 1
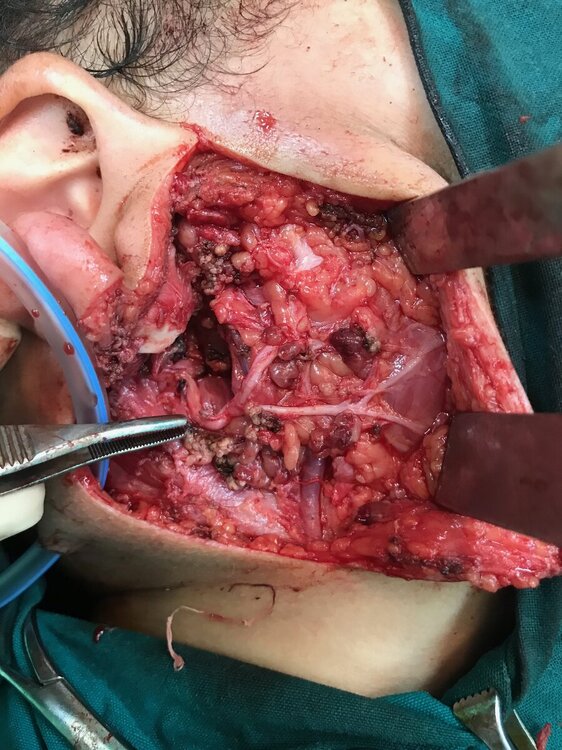
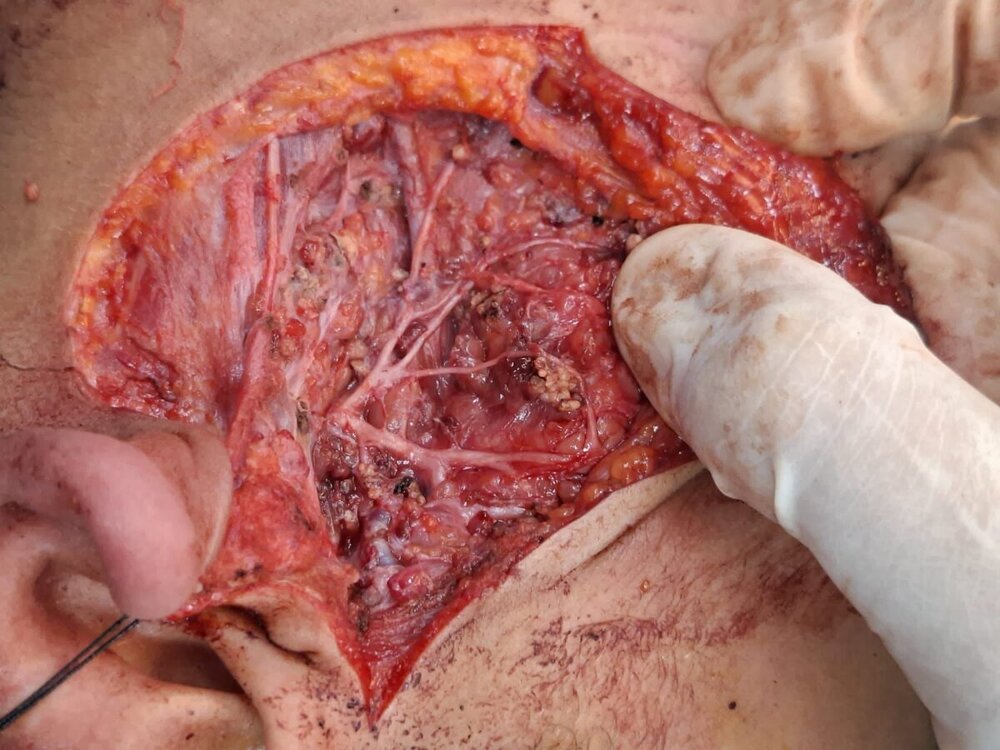
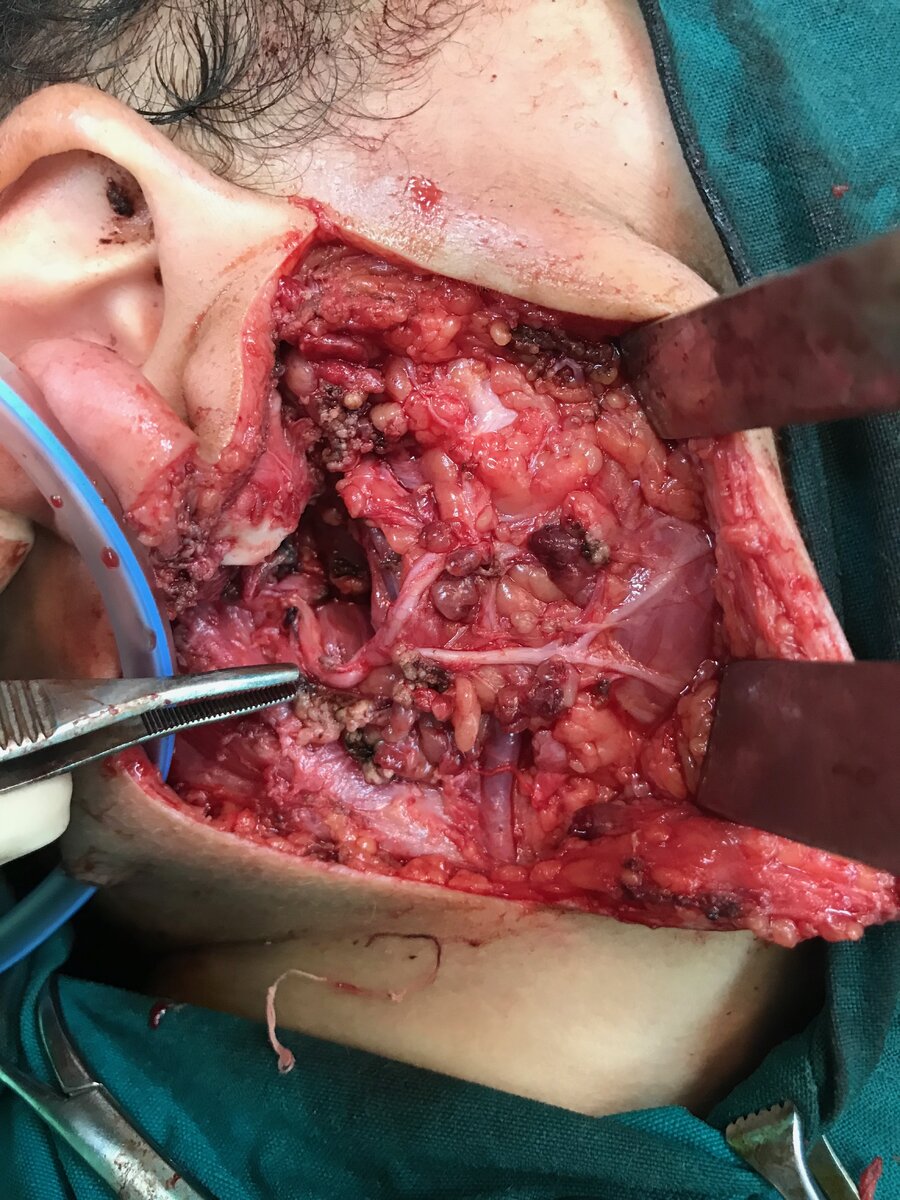
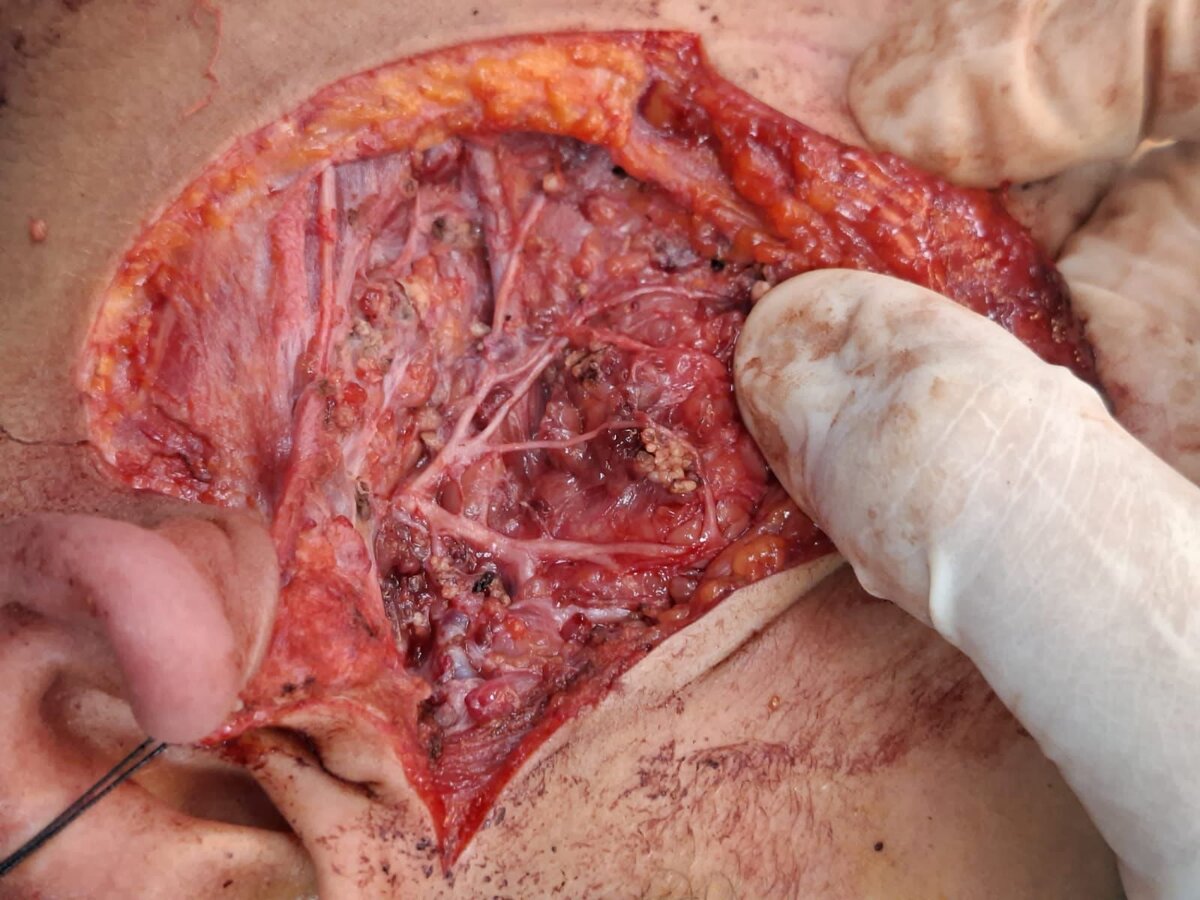
quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Hydrometrocolpos presents at the two extremes of childhood: initially during the neonatal period, when there is a high level of maternal hormones, and then at early puberty, when the patient herself begins to have production of estrogenic hormones. The distal vaginal obstruction is mostly due to imperforate hymen (in two thirds of cases), followed by a transverse vaginal septum and less commonly, vaginal atresia (with or without persistence of a urogenital sinus or cloaca)." "Associated anomalies are common and quite often severe. These include anorectal malformations and unilateral or bilateral agenesis of the kidneys, ureters, and trigone. Ultrasonography, micturating cystourethrography (MCU), and MR urography can help to evaluate the associated genitourinary anomalies."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Several problems have been encountered during the establishment of the ACE. The most common is pain during the washout, which is reported in up to 60% of patients. This usually settles spontaneously during the first 3 months but can be helped by reducing the concentration of the phosphate, reducing the rate of the infusion, or using an antispasmodic prior to the enema (such as Colofac, Solvary, UK). Despite regular washouts, patients may still become constipated, which also produces pain and should always be excluded. One of the other problems encountered is the time taken for the enema to pass and achieve a result; this has been a significant contributory factor to failure. The placement of the conduit in the distal descending colon has improved this situation considerably. Patients in whom the standard caecal ACE did not work have achieved excellent results with the left colonic ACE."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "None of our patients have needed secondary augmentation because of increased contractile activity. Even after the ileal segment is isolated from the gastrointestinal tract, it retains its absorption and secretory properties. As a result of the electrolyte exchange, hyperchloremic metabolic acidosis may develop. The extent of the electrolyte exchange depends on the amount of intestinal surface area in contact with urine and the time that the urine remains in contact with the intestine. Patients with normal renal function prior to augmentation have adequate compensatory mechanisms and do not have significant problems with acute metabolic changes. Patients who develop persistent, severe metabolic changes must be evaluated for insufficient bladder emptying. Another concern in these patients is a possible increased incidence of urinary tract infection (UTI), as bacterial flora from the augmentation may colonize the urinary tract. In recent years, we have used in our patients daily irrigation of the augmented bladder with 30 mL of 120 mg gentamicin per 250 mL of normal saline, and have found a low incidence of UTI with no evidence of gentamicin absorption or renal function deterioration."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "The site of the stoma on the skin is selected entirely for the patient’s convenience. The umbilicus provides a good passage and the best cosmetic result, but it is not an option in exstrophy patients. With patients in wheelchairs, the spine tends to become twisted with time, causing progressive abdominal compression, and the abdomen becomes hidden from the patient’s field of vision. For these patients, a stoma site close to the xiphisternum is the best option."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Augmentation cystoplasty is now commonly performed at most pediatric urological centres. Bladder augmentation has three major goals: to provide a compliant bladder reservoir, to limit bladder contractility, and to increase bladder capacity. Augmentation cystoplasty should allow the urinary tract to remain intact while preserving renal function and providing urinary continence. Various substrates are utilized to augment the bladder; the most commonly used is a segment of ileum, but stomach and large bowel also have been used. Ileum has been demonstrated to be the least contractile segment and therefore has become the tissue most often used for bladder augmentation. Sufficient augmentation should lead to effective bladder capacity."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Successful initial closure of the bladder and posterior urethra is the most important factor for achieving urinary continence and sufficient bladder capacity. The fragile mucosa and the detrusor function are best preserved by closing the bladder in the newborn period, but the size and the functional capacity of the detrusor muscle are important considerations for the outcome. Therefore, in the rare presence of a small, fibrotic bladder patch without elasticity or contractility, the operation should be deferred until adequate growth of the bladder template occurs. The risk of bladder neck failure is higher for the group with smaller bladder capacities (<100 mL). If sufficient size is not reached 4–6 months after birth, alternative options like creation of a colon conduit or ureterosigmoidostomy must be employed. Later in life, the former urinary diversion can be converted into a continent catheterizable pouch bladder or augmented bladder if the template is still intact."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Before the operation, the bladder capacity is measured annually by gravity cystograms with the child in anaesthesia. A bladder capacity of 100 mL or more is necessary to undergo bladder neck reconstruction. All children undergo an intense voiding training program, along with urodynamic evaluation, prior to the reconstruction."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "The ureteral stents are left in place for 10–14 days, and the suprapubic tube is removed 4 weeks postoperatively, after calibrating the bladder outlet to warrant free drainage. Note that the urethra is not stented at the end of the operation to avoid pressure necrosis, infection, and secretion accumulation. The pelvis is approximated in the midline by gently applying pressure over the greater trochanters bilaterally. Horizontal mattress sutures of #2 nylon are placed in the pubis. It is important to tie the knot away from the neourethra to avoid material migration into the posterior urethra. A second stitch of #2 nylon is used at the most caudal insertion of the rectus fascia onto the pubic bone for added security, if it can be easily done and does not compromise the first stitch."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "The operations are performed with general anaesthesia, with the patient in a supine position even for the osteotomies. A tunneled epidural catheter is placed when possible to reduce the intraoperative amount of anaesthetic agents and for postoperative pain control. It is typically left in place for several weeks after the closure. Care must be taken to create a latex-free environment in the operation room, as many children with bladder exstrophy are prone to latex allergies. Perioperative broad-spectrum antibiotics are administered and continued throughout the first postoperative week."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Combined exstrophy and epispadias repair: In a few selected cases, newborn exstrophy closure can be combined with epispadias repair. This approach requires good phallic length, a deep urethral groove, and an adequate amount of penile skin, however, and it should be attempted only by experienced exstrophy surgeons, as the complications can be severe. Combined exstrophy and epispadias repair is best applied in the patient undergoing delayed primary or reoperative exstrophy closure. The preoperative use of intramuscular testosterone in reoperative exstrophy patients will allow for improved vascularity and more penile skin for the reconstruction."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "pelvic osteotomies are performed if the patient is older than 72 h, for a symphyseal diastasis of more than 4 cm or if a tension-free closure cannot be achieved. In those cases, osteotomies are crucial to ensure tension-free approximation of the bladder, posterior urethra, and abdominal wall, preventing dehiscence or bladder prolapse. Furthermore, it places the urethra deep within the pelvic ring, enhances bladder outlet resistance, and ensures alignment of the large pelvic floor muscles to support the bladder neck."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Achieving urinary continence with a sufficient bladder capacity is strongly dependent on initial successful closure of the bladder and the posterior urethra as well as the size of the bladder template. Therefore, the first step of the reconstruction is conversion of bladder exstrophy into a penile epispadias with incontinence with a balanced posterior outlet resistance that preserves renal function but stimulates bladder growth."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "The technique includes early closure of the bladder, posterior urethra, and abdominal wall, usually with pelvic osteotomy in the newborn period, subsequently followed by an early epispadias repair at 6 months to 1 year of age after testosterone stimulation by intramuscular injection. Around age 4–5 years, when adequate bladder capacity is reached and the child is ready to participate in a very structured preoperative and postoperative voiding program, a competent bladder neck is reconstructed, with bilateral ureteral reimplantation."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Ureteral reflux in various degrees is seen in 100% of cases after closure. A preoperative ultrasound evaluation of the otherwise usually unaffected upper tracts is mandatory to determine the presence of two normal kidneys"video 1 quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "The confluence is not always readily apparent, especially in very masculinized patients who have a UGS resembling a male urethra. In these patients, one must actively look for a verumontanum-like structure with a small “utricular” opening in the proximal urethra. This is the confluence. A guidewire or ureteral catheter should be inserted into this communication through the cystoscope, and then the scope can be passed over the guide into the vagina. In almost all cases, we find it helpful to place a Fogarty catheter into the vagina and inflate the balloon (Fig. 68.1). Even in the smallest neonate, this can be done by passing the Fogarty catheter through the cystoscopic sheath and clamping the catheter with a hemostat after the balloon is inflated."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Rink et al. described the “PVE” classification, in which the length and width of the phallus (P) is measured in centimeters, the location of the vaginal confluence (V) is recorded in centimeters from the bladder neck and from the UGS opening, and the degree of masculinization of the external genitalia (E) is estimated with a Prader number of 1–5."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "The testis fails to remain in the scrotum in a significant number of older boys. They appear to have acquired cryptorchidism, which has been called ascending testis, gliding testis, or pathologically retractable testis. The abnormality is likely secondary to failure of the spermatic cord to elongate in proportion to the boy himself. (The spermatic cord length doubles from 5 cm to 8–10 cm in the first 10 years after birth.) At surgery, the major finding is a fibrous remnant of the obliterated processus vaginalis, linking acquired UDT with inguinal hernia. Occasionally the processus is still patent as a latent hernia. The indication for surgery in this acquired group is failure of the testis to remain in the scrotum without traction."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Consensus is building that the crucial step in postnatal germ cell maturation is transformation of neonatal gonocytes into type A spermatogonia in the second 6 months after birth; hence the current recommendation for orchidopexy is at 6 months of age. Prevention of germ-cell loss is the aim of surgery, although this effect remains unproven."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Circumcision of the visible external prepuce in these cases does not achieve emergence of the penis and may compromise the eventual reconstruction of a more normal circumcised appearance. An operation for this condition, to release the tethered corpora and remodel the shaft skin,"quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "The buried penis is an abnormality of peno-scrotal fusion, in which the penile corpora are also tethered to the deep fascia of the lower abdominal wall. It is associated with phimosis, and the appearance of the external skin suggests that the penis is small or even absent. Often the inner preputial space is enlarged and balloons during voiding, with dribbling from the preputial orifice—referred to as megaprepuce."Collection of superficial parotidectomy operative photos from colleagues at Pediatric surgery unit, Menofia university hospitals, Egypt
quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "The confluence is not always readily apparent, especially in very masculinized patients who have a UGS resembling a male urethra. In these patients, one must actively look for a verumontanum-like structure with a small “utricular” opening in the proximal urethra. This is the confluence. A guidewire or ureteral catheter should be inserted into this communication through the cystoscope, and then the scope can be passed over the guide into the vagina. In almost all cases, we find it helpful to place a Fogarty catheter into the vagina and inflate the balloon (Fig. 68.1). Even in the smallest neonate, this can be done by passing the Fogarty catheter through the cystoscopic sheath and clamping the catheter with a hemostat after the balloon is inflated."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Rink et al. described the “PVE” classification, in which the length and width of the phallus (P) is measured in centimeters, the location of the vaginal confluence (V) is recorded in centimeters from the bladder neck and from the UGS opening, and the degree of masculinization of the external genitalia (E) is estimated with a Prader number of 1–5."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "The testis fails to remain in the scrotum in a significant number of older boys. They appear to have acquired cryptorchidism, which has been called ascending testis, gliding testis, or pathologically retractable testis. The abnormality is likely secondary to failure of the spermatic cord to elongate in proportion to the boy himself. (The spermatic cord length doubles from 5 cm to 8–10 cm in the first 10 years after birth.) At surgery, the major finding is a fibrous remnant of the obliterated processus vaginalis, linking acquired UDT with inguinal hernia. Occasionally the processus is still patent as a latent hernia. The indication for surgery in this acquired group is failure of the testis to remain in the scrotum without traction."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Consensus is building that the crucial step in postnatal germ cell maturation is transformation of neonatal gonocytes into type A spermatogonia in the second 6 months after birth; hence the current recommendation for orchidopexy is at 6 months of age. Prevention of germ-cell loss is the aim of surgery, although this effect remains unproven."quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "Circumcision of the visible external prepuce in these cases does not achieve emergence of the penis and may compromise the eventual reconstruction of a more normal circumcised appearance. An operation for this condition, to release the tethered corpora and remodel the shaft skin,"quote from "Pediatric Surgery (Springer Surgery Atlas)" by Prem Puri, Michael E. Höllwarth - "The buried penis is an abnormality of peno-scrotal fusion, in which the penile corpora are also tethered to the deep fascia of the lower abdominal wall. It is associated with phimosis, and the appearance of the external skin suggests that the penis is small or even absent. Often the inner preputial space is enlarged and balloons during voiding, with dribbling from the preputial orifice—referred to as megaprepuce."Collection of superficial parotidectomy operative photos from colleagues at Pediatric surgery unit, Menofia university hospitals, Egypt